




















Varicose veins are a pathological and irreversible change in the walls of peripheral veins with incompetence of the valve apparatus and impaired blood flow.Veins of different locations are subject to varicose transformation, but the vessels of the superficial venous network on the legs are most often affected, so varicose veins most often indicate a disease of the veins of the lower extremities.
How do varicose veins appear?
In the case of varicose veins, only the peripheral superficial venous vessels undergo pathological transformation - this is due to the structural characteristics of the walls and the physiology of blood outflow from the extremities.It is these pathogenetic moments that are decisive.All other predisposing factors affect the entire vascular system, but do not lead to characteristic changes in central veins and arteries of any caliber.
Let's consider the pathogenesis of varicose veins:
- Aseptic inflammation. It starts from the endothelium of the veins, and then spreads to the entire thickness of the vessel.The triggering mechanism in most cases is the slowing down of blood flow;there is a parietal grouping of cellular elements of the blood with rolling of leukocytes - grouping and "rolling" of leukocytes along the surface of the endothelium.Over time there is a tendency for them to adhere, which causes the release of inflammatory mediators.There are still no external changes at this stage.
- Remodeling of superficial vein walls and valves. It leads to changes in density and elasticity.Aseptic inflammation, genetic defects of connective tissue proteins, mechanical microdamages of the endothelium and some other factors contribute to this.In affected vessels, the ability to reversibly compensate for fluctuations in venous pressure is significantly reduced and they become rigid.
- Persistent and progressive expansion of the lumen of the affected veins. These changes are initially quite local;then the pathological process spreads not only along one vessel, but also includes other components of the peripheral venous network.
- Compensatory lengthening of the affected vein with the formation of pronounced pathological bends. Characteristic bulging nodes are formed, which give the disease its name: "varix" is translated from Latin as "swell".
- Development of valvular insufficiency. Functional stoppage of the valves in the lumen of the affected superficial veins with reversed blood flow (vertical reflux).In the beginning, it is relative in nature and is manifested only by a noticeable increase in peripheral venous pressure.After that, the failure becomes absolute - the valve walls do not close completely under any conditions.Venous stagnation (blood stagnation) occurs with the formation of venous insufficiency.
- Involvement of perforating veins in the process.They are also called communicative or commissural.Their pathological expansion is accompanied by valve insufficiency, which contributes to the pathological flow of blood from the deep venous network to the superficial (horizontal reflux).Increased venous insufficiency.
All these changes are irreversible and last even with the complete elimination of provoking and predisposing factors, therefore it is impossible to cure already developed varicose veins with conservative methods;it is only possible to partially compensate for the disturbances for some time.
Causes of varicose veins
Varicose veins are a polyetiological disease whose development is triggered by external and internal (endogenous) factors.The main reasons for the development of varicose veins:
- Hereditary factor.
- Poor mobility, prolonged sitting.
- In women - changes in hormonal status during pregnancy, taking oral contraceptives and carrying out hormone replacement therapy.
- Conditions accompanied by partial compression of the pelvic veins: pregnancy (especially multiple pregnancy or occurring with polyhydramnios), mass formations in the abdominal cavity, some intestinal diseases.Constipation and chronic lung diseases with cough, which lead to an increase in intra-abdominal pressure, lead to venous outflow disorders at the level of the pelvis.
- Increased body weight.
All people are predisposed to developing varicose veins.This is due to the vertical position of the body, due to which, under the influence of gravity, the blood tends to the distal parts of the lower extremities, and the veins experience increased stress and are more easily deformed.
Symptoms and manifestations of varicose veins
Symptoms of varicose veins of the superficial veins of the thighs and legs include:
- Visible changes in the affected veins.Varicose veins are tortuous, excessively shaped, dark, visible through the skin and bulging.Pulsation is not characteristic for them.As the disease progresses, local nodular bulging formations appear on the legs, which often form entire conglomerates and do not disappear completely when lying down.In patients with increased body weight, changes in the veins often remain practically imperceptible for a long time, masked by excessive subcutaneous fat.
- Swelling of feet and legs after prolonged standing and sitting, in the evening, when staying in conditions of elevated ambient temperature.Such venous edema is not accompanied by cyanosis of the distal extremities, which can be observed in heart failure.They decrease and even disappear after rest (including a night's sleep), when the legs are kept in an elevated position, after performing special gymnastics to activate the "muscle pump" of the lower leg.Swelling is one of the first signs of chronic venous insufficiency with varicose veins.
- A feeling of heaviness and fullness in the legs, even in the absence of obvious swelling.Such complaints occur in conditions that promote pathological blood deposition in the distal parts of the lower extremities.The discomfort most often occurs in the evening and after a long stay in an upright position with little physical activity.
- Signs of ischemia of the muscles of the extremities affected by varicose veins: increased muscle fatigue, sometimes cramps.
- Unpleasant sensations in the legs, which usually increase with increasing swelling due to the reaction of soft tissues and peripheral nerve branches of the legs to compression by excess intercellular fluid.Another possible cause of such paresthesias are dysmetabolic trophic disorders.
- Visible trophic disorders of the skin and underlying soft tissues.These can be dry or eczematous dermatitis, hyperpigmentation, lipodermatosclerosis (thickening, hardening of the dermis and tissues), ulcers.
Symptoms of varicose veins of the lower extremities appear quite early, although not all patients pay attention to them in time.The order in which new features are added may vary.In some patients, an aesthetic defect is initially observed in the form of clearly altered veins, while in others the disease appears in the form of venous insufficiency.
Phases
The stages of varicose veins are determined according to the CEAP classification:
- C0—no signs of pathology;
- C1—presence of reticular varicose veins or telangiectasias;
- C2 - varicose veins;
- C2r - recurrent varicose veins;
- C3 - swelling of the extremities;
- C4a - trophic changes: hyperpigmentation or venous eczema;
- C4b - trophic changes in the form of lipodermatosclerosis or white skin atrophy;
- C4c - corona venosus foot;
- C5—extended trophic ulcer;
- C6 - open trophic ulcer.
- C6r – recurrent open trophic ulcer.
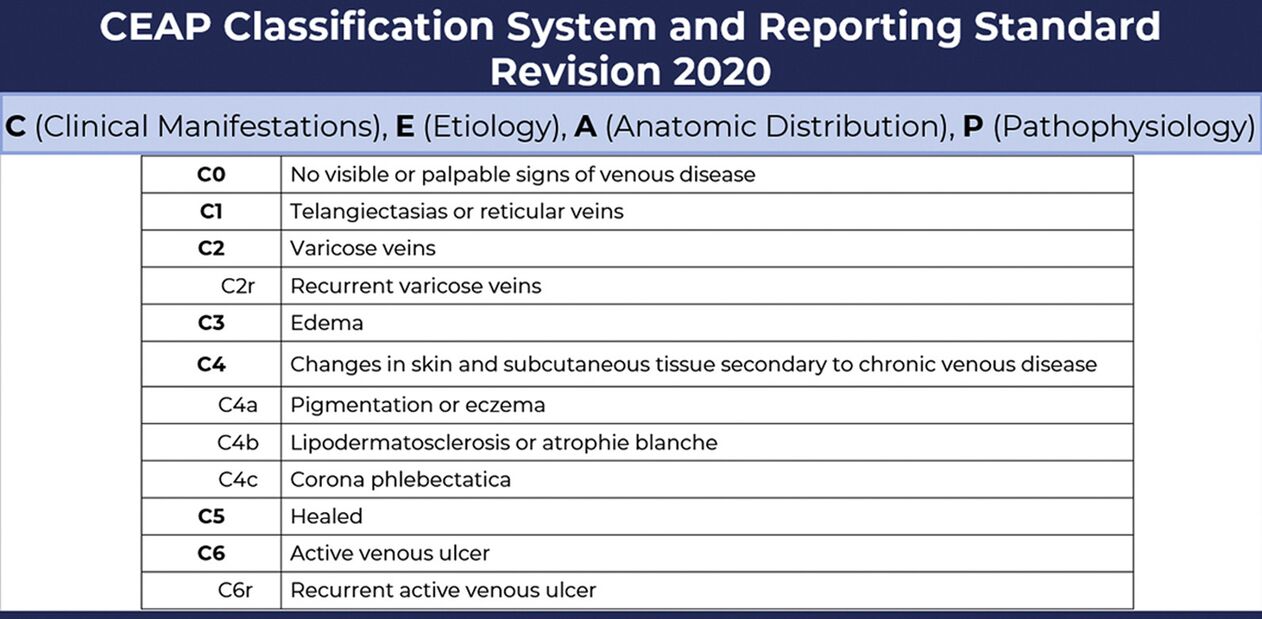
The CEAP classification was created in 1994 and is now international and generally accepted.It is used by phlebologists when making a diagnosis.
For example, in class C1, only a cosmetic defect is noted - dilated reticular veins of about 1 mm.in diameter, and with C4c it is no longer possible not to notice serious trophic disturbances.


%20and%20reticular%20veins.jpg)

Diagnostics
A basic examination to confirm the diagnosis of varicose veins of the lower extremities and to clarify the extent and nature of the disorder includes:
- Clinical examination.A phlebologist determines the flow and condition of visible superficial veins, changes in the skin and soft tissues, the presence of edema.Functional tests are performed to assess vertical reflux and determine the approximate level of horizontal reflux.The patient survey aims to clarify the predisposing and provoking factors, the duration and characteristics of the development of the disease.
- Ultrasound examination.In the case of varicose veins, the most informative is not a conventional ultrasound, but an assessment of blood flow using Doppler Doppler ultrasound (USD).The study shows the speed of blood movement, the presence of pathological venous-venous reflux and impaired vascular patency.This information is necessary so that the doctor can choose the necessary treatment regimen.
- Hemostasiogram (blood tests for a comprehensive assessment of the coagulation system).

According to the indications, a multi-layer computed tomography (MS CT) is performed - a high-tech study in some cases becomes the main technique for determining the image of damage to the venous system.
In modern medicine, other diagnostic techniques are also used - plethysmography, laser Doppler flowmetry.They are not available to a wide range of patients;the obtained results are usually not critical in determining treatment tactics.Usually, a basic examination is sufficient, which is complemented, if necessary, by consultations with specialists (endocrinologist, hematologist, cardiologist and others).Previously, several stages of varicose veins of the legs were distinguished.Currently, when making a diagnosis, phlebologists use the CEAP classification of chronic venous diseases, which includes the characteristics of the case according to clinical, etiological, anatomical and pathophysiological characteristics.
The danger of varicose veins
Many people believe that varicose veins of the lower extremities are mainly a cosmetic problem.Indeed, often the external unattractiveness of legs with knotty, bulging blue-purple veins or spider veins is the main reason for a visit to the doctor.
Pathologically enlarged peripheral veins are a condition that should not be underestimated.It can significantly worsen the patient's well-being and even lead to life-threatening complications.And that is primarily due to the development of chronic venous insufficiency due to persistent and progressive hemodynamic disorders.Other unpleasant consequences are also possible.
Consequences of advanced varicose veins:
- Significant deterioration of the patient's quality of life.Significant discomfort and even reduced performance in varicose veins are caused by heavy leg syndrome, swelling, night cramps, poor healing and recurrent ulcers.
- Changes in soft tissues with a decrease in the external attractiveness of the legs, which is especially important for women.Moreover, hyperpigmentation, lipodermatosclerosis and traces of healed ulcers usually persist even after the removal of the affected veins, especially if the surgical treatment was carried out against the background of already developed pronounced trophic disorders.
- Bleeding from ruptured dilated nodes or veins at the base of trophic ulcers.
- Development of thrombosis and thrombophlebitis of superficial veins.It is burdened not only with local hemodynamic disorders and inflammation, but also with distant thromboembolism with infarction of various organs and acute life-threatening conditions.
- Deep vein thrombosis is an even more dangerous condition in terms of thromboembolism.
Already developed complications of varicose veins of the superficial veins of the thighs and legs not only negatively affect the patient's condition and the prognosis of the disease.They significantly reduce the probability of obtaining a quick and sufficient result even when radical methods of treatment are used.
Is the disease always dangerous?
Varicose disease of the lower extremities with valvular insufficiency of the saphenous veins is not the only possible variant of this pathology.There is also a so-called "cosmetic" version of varicose veins.According to the classification of chronic venous diseases, CEAP is C1, the characteristics of the form:
- Damage to small intradermal vessels up to 3 mm in diameter.They can be subepidermal or reticular.
- The appearance of spider veins, reticular dilated veins in the form of a fine surface network.
- Absence of vertical or horizontal pathological venous reflux.Affected small vessels do not have valves and communicate only with small saphenous vein tributaries by means of feeding pedicles.They collect blood from certain sectors of the dermis and take it to larger, deeper vessels.Disturbance of blood flow at this level does not contribute to the development of chronic venous insufficiency.
This course of the disease does not lead to the development of clinically significant complications.In fact, patient discomfort is a consequence of a cosmetic defect.But this does not mean that a person with the presence of spider veins is excluded from damage of larger caliber veins.In such a situation, C1 is no longer diagnosed, but C2 and the following classes according to the CEAP classification.
Treatment of varicose veins
Treatment of varicose veins should not begin with the development of complications, but in the phase of primary changes and minimally expressed signs of venous insufficiency.You can expect a quick onset of the expected effect, a complete regression of symptoms and a low probability of relapse.Treatment of advanced varicose veins will not be as effective.Sometimes his task will be only to reduce the speed of disease progression, create conditions for healing trophic ulcers and reduce the severity of chronic venous insufficiency.
In general, all methods of treating varicose veins of the lower extremities can be divided into non-surgical (conservative) and surgical (radical).Traditionally, most patients prefer gentle techniques, delaying the decision to operate until uncorrectable complications develop.And many of them do not even consult a doctor, they resort to self-medication.Self-medication often leads to complications of the pathology.
Conservative treatment
A conservative treatment regimen for varicose veins includes:
- Systemic drug therapy.Aimed at improving the rheological properties of blood to prevent thrombosis, achieve anti-inflammatory effects, increase the elasticity of the vascular wall and stimulate tissue regeneration.
- Local drug therapy (ointments, creams, gels).External means are intended to improve microcirculation, reduce swelling, increase vein tone and treat trophic ulcers.
- Therapeutic exercise increases the efficiency of the lower leg muscle pump and thereby improves blood flow from the legs.
- Use of compression stockings.Compression stockings and tights provide dosed compression of superficially located veins, which reduces the tendency for blood to settle and edema, improves well-being and reduces the likelihood of thrombosis.
- Physiotherapy.They are used mainly in the absence of open trophic ulcers and beyond the acute stage of thrombophlebitis.Hardware pneumocompression, darsonvalization, galvanization, UHF therapy, UV therapy, hydrotherapy and ozone therapy are used.The goals of physiotherapy are to improve venous and lymphatic drainage, improve microcirculation, stimulate regeneration and reduce the severity of complaints.

Medicines will not restore healthy blood flow to already damaged veins;they will remain tortuous and expanded.Even a slight increase in the tone of the vascular wall under the influence of phlebotonics will not be able to completely correct valvular insufficiency.
One should not expect high results from conservative treatment.It will reduce pain and swelling, reduce the risk of thrombosis and improve the healing of trophic disorders.But it is impossible to save the patient from varicose veins and prevent further progression of the disease with a conservative approach.
Surgical treatment
The invasive (surgical) method of treating varicose veins aims to exclude the affected vessel and its main tributaries from the general blood flow (by removal or obliteration) and eliminate horizontal venous reflux.It does not worsen tissue ischemia, improves trophism by significantly reducing (or even eliminating) the venous path.This treatment not only eliminates the cosmetic defect, but also helps in dealing with chronic venous insufficiency.
Classic surgical methods for the treatment of varicose veins of the lower extremities:
- A crossectomy is a complete section of a ligated large superficial vein at the point where it flows into the deep venous network.
- Phlebectomy – removal of a superficial vein affected by varicose veins (great or small saphenous).It is performed by removing (pulling out, pulling out) the vessel using instruments through small incisions.It is currently combined with crossectomy and tributary removal.
- Miniphlebectomy – removal of large perforators and tributaries through small incisions or punctures.
For a long time, the main method of surgical treatment was open surgery, their disadvantages:
- Significant blood loss;
- Bleeding in the area of surgery, sometimes requiring repeated operations to evacuate the blood.
- Lymphostasis due to the crossing of lymphatic vessels.
- Severe pain syndrome.
- Long-term disability.
A modern alternative to surgery
Endovascular techniques are considered minimally invasive interventions;they do not require incisions.They are not so traumatic and are not inferior in efficiency to classical operations.Complications and recurrences after them are less frequent than after operations.
Minimally invasive methods:
- Laser obliteration
- Sclerotherapy/Cryosclerotherapy
- Radio frequency obliteration.
In minimally invasive methods, the vein affected by varicose veins is not removed, as in classic operations.Its wall is exposed from the inside with laser or radiofrequency energy, and during sclerotherapy with a sclerosant.This provokes "sticking" of the vessel and its subsequent fibrosis and replacement by connective tissue.This closure of the lumen of the vessel is called obliteration.And with RFM stars, they are actually vaporized under the influence of radio frequency waves.